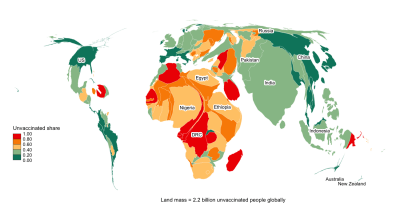
Global challenges require global solutions. So the dictum goes. Yet, here we are: while the richer part of the world has made considerable progress with primary COVID-19 vaccinations and is advancing on boosters, most people in the poorest countries still lack their first shots and boosters are quasi inexistent. Moreover, the shots given so far – be it primary or booster – would not even be sufficient to protect the tiny groups of elderly cohorts and health workers in these demographically very young countries. This sheer inequality is epidemiologically wrong, it is socio-economically wrong and most of all it is morally wrong. Vaccine equity needs a boost.
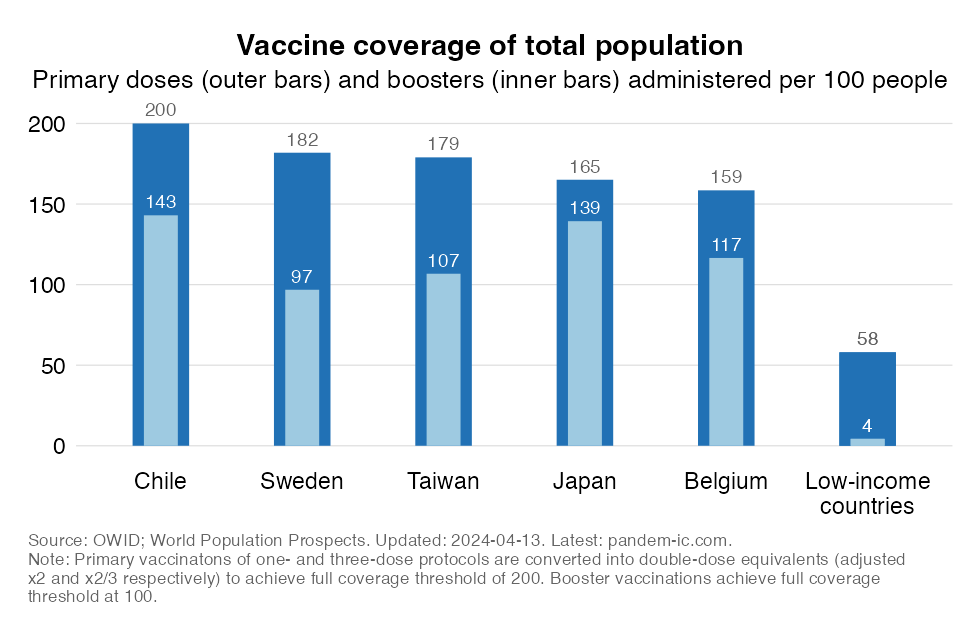
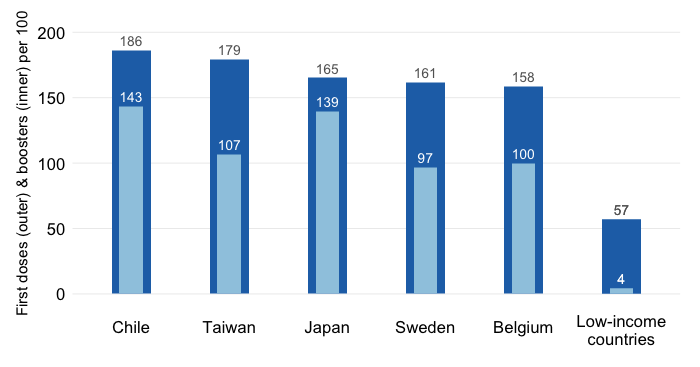
The chart illustrates the contrast at its most extreme as we compare LICs with the best performers on boosters. Let’s briefly explain what is being displayed:
Booster coverage (inner bars) is also per 100 people, where booster doses are unadjusted for vaccine protocol. Note that due to a lack of comprehensive data at the global level we are unable to differentiate between initial and subsequent booster cycles.
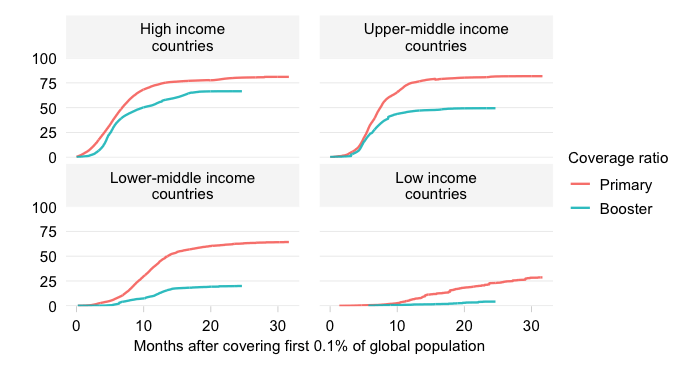
The above is an extreme comparison that highlights the sheer contrast between the best performers and the group of worst performers. Let us now look at this more generally and consider the world together with the four groups of the full World Bank income classification. Note that in the chart below bars will refer to primary coverage and dots to booster coverage.
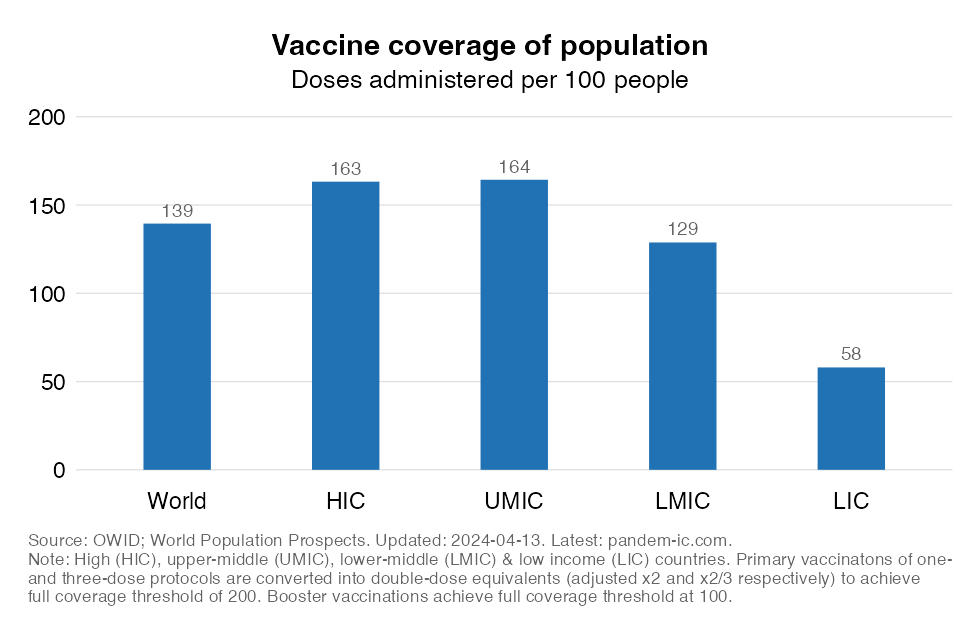
The global picture remains bleak:
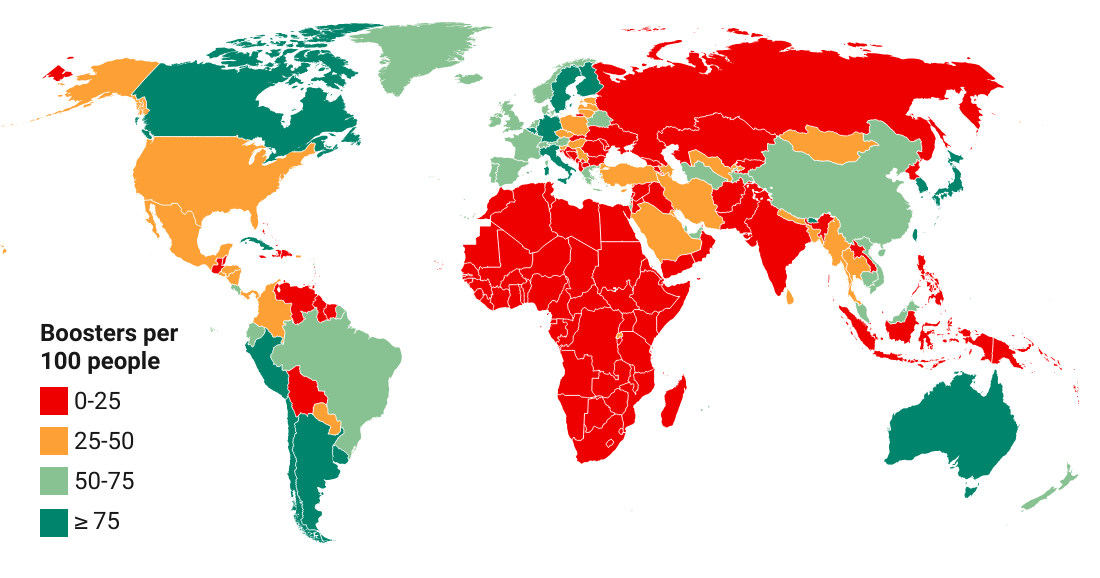
On booster coverage, we see a similar pattern. HICs and UMICs have similar booster rates that are reasonably well elevated. But LMICs and LICs who comprise the poorer half of the world have made much less headway on the booster front. That of course is partly a derivative of the progress on the primary series. But it is still striking how low coverage ratios are for boosters.
Let us now examine the vaccination progress made thus far through the lens of the ability of countries to cover their priority group – those who governments would wish to vaccinate first on account of their exposure to infection or vulnerability to severe disease once infected.
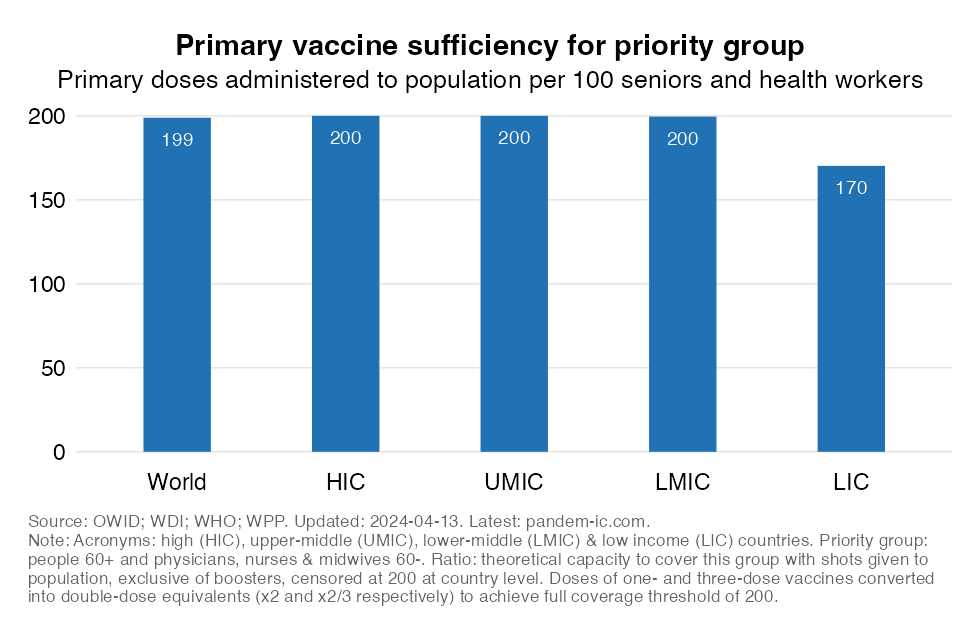
The above chart shows where we are with regard to the primary series. Luckily by now, the supply of vaccines (as revealed, admittedly imperfectly, by the number of doses actually administered) suffices to cover almost everyone in our pragmatic definition of the priority group. There are however still significant shortages in the group of LICs.
To reiterate, note that we are not saying that the global priority group has in fact been covered as well as is indicated here – that unfortunately does not turn out to be the case as this post shows. No, we are saying that the supply of vaccines appears to have been sufficient to cover them well – i.e. as per the full protocol. In other words, any persistent deficiencies in vaccine coverage likely derive from factors such as lack of prioritization of the priority group, differences in definition of the priority group or demand-side factors such as hesitancy.
We will now repeat the analysis for booster coverage. In the chart below, we assess to what extent the global priority group could have been covered if the boosters administered thus far had been prioritized towards them.
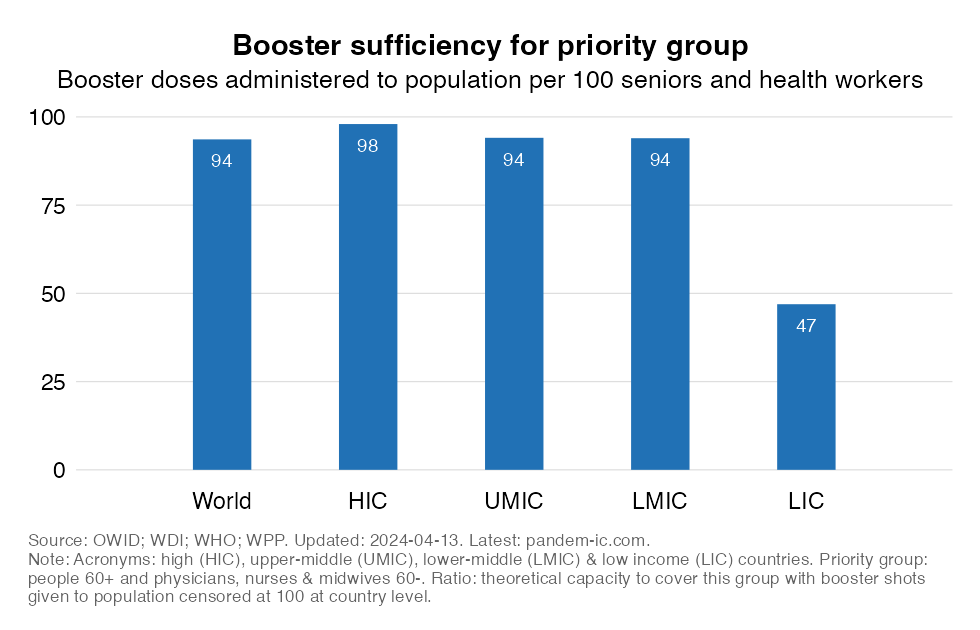
The results show that the world is, on average, in a good spot when it comes to booster sufficiency. But, again, there is one important exception: the group of LICs.
The charts above tell a story of progress but they also indicate that the world continues to fall considerably short of an equitable outcome.
Enough vaccines should theoretically be available to cover priority groups with primary shots and boosters. But that does not turn out to be the case for LICs. From a population-level vaccine coverage perspective, the gaps in primary vaccination remain considerable. and booster vaccination has yet to take off. LMICs are in a better position than LICs, but even in these countries the gaps remain very large.
These outcomes are not justifiable – neither epidemiologically, socio-economically or, most importantly, morally. Yes, the reasons for low uptake in poorer countries are multiple, but vaccine equity remains an issue that permeates the demand and supply side of the equation. And this is not to mention the lack of equity in other dimensions of global health and beyond that manifest themselves indirectly in demand and supply decisions.
Vaccine equity continues to be in need of a boost!
Disclaimer: Posts by the Center for Global Development reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. Likewise, views expressed do not necessarily reflect those of the United Nations, the United Nations Development Programme, its programmes/projects or governments. The designations employed do not imply the expression of any opinion whatsoever concerning the legal status of any country, territory or area, or its frontiers or boundaries.