The Top 5 for excess mortality during the first two years of the pandemic were India, Russia, Indonesia, USA and Brazil (in that order). These are the results based on cumulative excess mortality as per the new database that was released by the WHO. We’ve analyzed this database in two related posts (here and here). What sets it apart from other sources is that the database provide detailed estimates by age cohort. In this post, we will review the performance of the Top 5 contributors to the global total.
Before we dive into the results by age cohort, let’s briefly review the excess mortality trends across the age distribution for the Big Five. India, Russia, Indonesia, USA and Brazil – in that order – were selected as they had the highest cumulative excess mortality count as of end 2021. The chart below shows the monthly evolution in that variable over the course of first two calendar years of the pandemic.
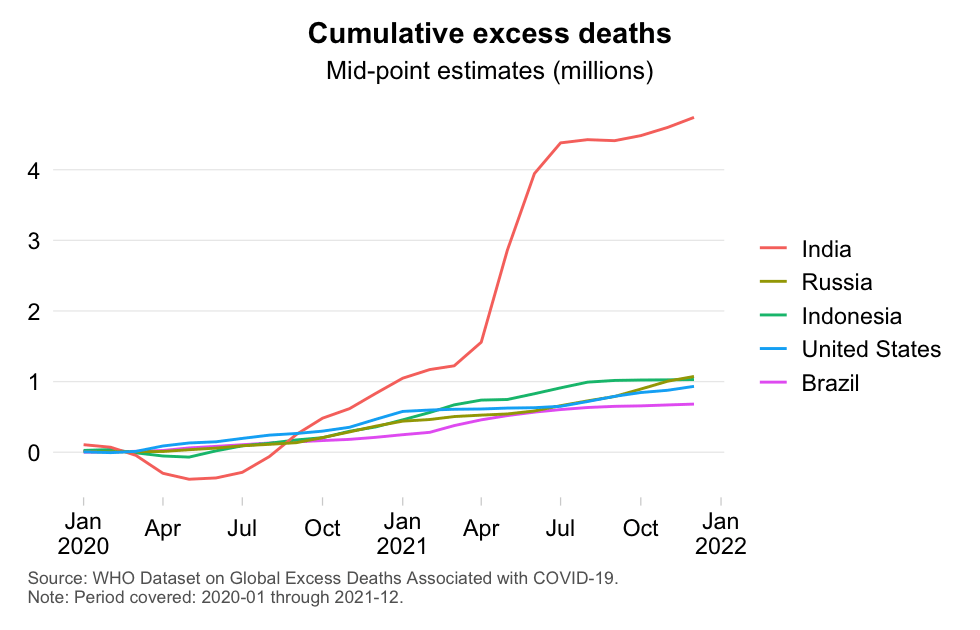
The chart reveals interesting results. First, note how India stands out. India saw a major escalation around May 2021 when excess mortality skyrocketed. The mid-point estimate end of 2021 was well over 4 million. This contrasts with the performance of the country in the first half of 2020 when excess mortality was estimated to be negative.
Second, Russia, Indonesia and the USA have roughly identical excess death counts, with Brazil following closely. These are of course all very populous nations so we expect them, all else equal, to contribute relative to their population share. Or better: relative to their elderly population share as we know that most of excess mortality has occurred in the elderly cohorts. Having said that, China has a larger elderly cohort (60+) than any of the Big 5 and Japan’s is bigger than that of Brazil and Russia. Yet, China and Japan do not feature in this list of the top 5 contributors to global excess mortality.
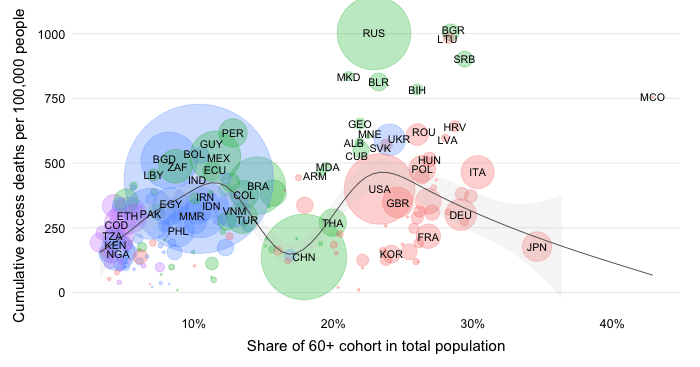
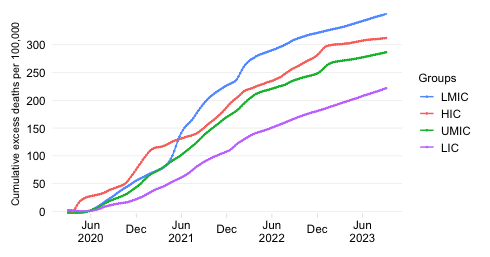
Let us now review the per capita numbers. The chart below shows the monthly evolution in the mid-point cumulative excess death estimates normalized by population (per 100,000 people).

What is remarkable is that India, despite its huge population, continues to have a very high excess mortality rate even on a per capita basis. Yet, it is not India that claims the top spot, but Russia. About 23% of the Russian population finds itself in the 60+ age cohorts, so Russia is a country with a large elderly population. Other factors will have played a major role in driving the high excess mortality rate as the US has a similar elderly share but less than half the excess mortality rate. Note also that India, Indonesia and Brazil have remarkably similar excess mortality rates despite being demographically very different, again pointing to other factors driving the results.
Let us now review the results by age cohort. We will also continue to differentiate by pandemic year, which the WHO’s dataset allows us to do. The chart below then presents the cumulative excess death estimates in the absolute by age cohort and year.
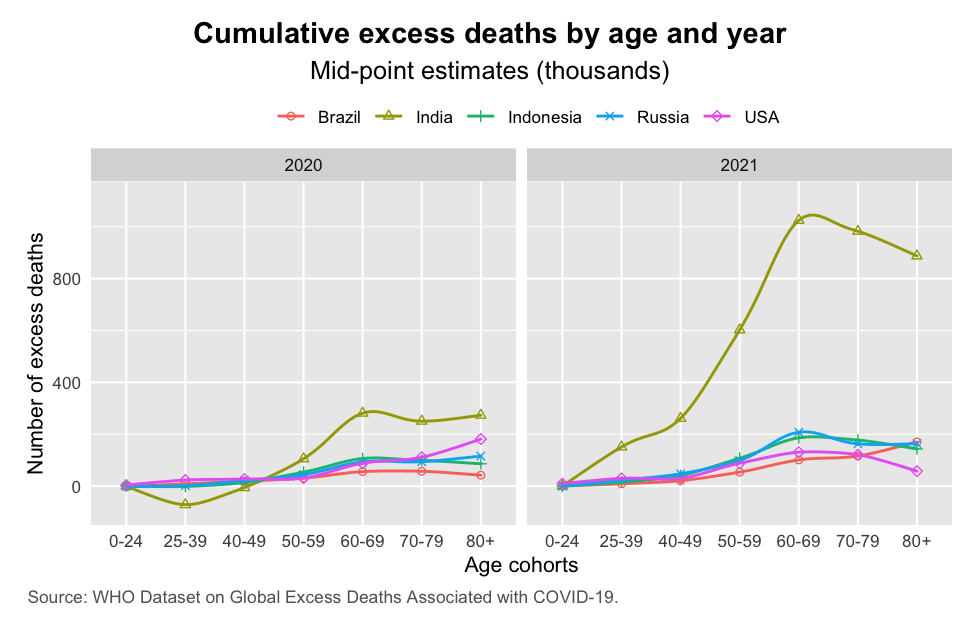
A few results are striking. First, note the general escalation of the pandemic between 2020 and 2021 and how much this was driven, across all age cohorts, by India. Second, note how the the elderly cohorts (above 60) registered much higher excess mortality during the second year. This is especially noticeable for India, but is also true for other countries. Interestingly, in the US, excess mortality in the 70-79 cohort seems to have been roughly stable while that in the 80+ cohort actually declined. Third, note also that the non-elderly cohorts saw a significant rise in excess mortality when we compare 2020 with 2021.
The next chart shows the per capita numbers for excess mortality by age. This is perhaps the best way to analyze pandemic performance as it controls for demographic structure. We would naturally expect that mortality rates of very young countries are different from those of older countries simply because COVID-19 is an age-discriminating disease that disadvantages the elderly.
The results by age cohort insulate mortality rates from differences in age structure and show how much more vulnerable the elderly cohorts have been in some countries. In some cases, age-specific vulnerability is so much higher that the overall demographic advantage of having a younger age structure is offset – a result that is discussed in more detail here.
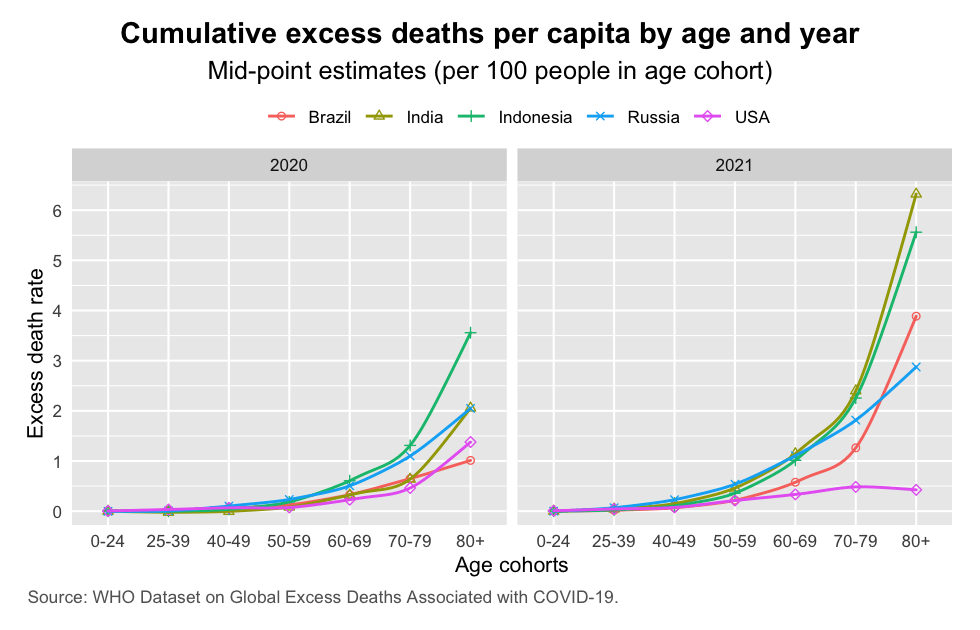
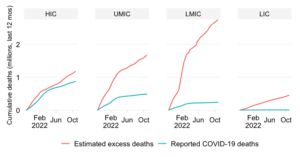
Two patterns are obvious. First, the age-specific excess mortality estimates show a considerable gap between the US – a high-income country – and the developing countries in this sample, where Brazil and Russia are upper-middle-income countries and India and Indonesia are lower-middle-income countries. Excess mortality rates do not exhibit a monotonously increasing relationship as we go from HIC to UMIC and from UMIC to LMIC in this sample as the 2020 data show. But in 2021 that is no longer the case and excess mortality becomes tightly related to the income classification.
Second, the gap between the US and other countries rose dramatically in 2021. This is related in large part to the US making more headway on the vaccination front. It is also related to the non-linear effects of a pandemic getting out of hand where the spread of infections overwhelms the capacity of hospital systems and medical supplies, such as oxygen.
Comparing outcomes in 2021 with the US, the elderly have suffered disproportionately especially in India and Indonesia but also Brazil and Russia. In India and Indonesia, alone, an estimated 1 out of 100 people in the 60-69 bracket are estimated to have passed away over and beyond what would have been expected under “normal conditions” (that’s the definition of excess mortality). The results are even worse for the outer age brackets: 2.5% in the 70-79 bracket and 6% in the 80+ bracket are estimated to have died.
These results illustrate what a carnage the pandemic has been in the developing world and how much the elderly cohorts have suffered. It underscores once again the need to focus on developing country impacts, which oftentimes get obfuscated by inequality in data quality (to put it euphemistically) as well as by the mistaken notion that mortality rates are low due to the large population sizes and young demographics. It also underscores the need to remain vigilant and accelerate and prioritize better vaccination so that these elderly cohorts can be better protected should a new wave and/or a new variant attempt to wreak havoc once again.
Disclaimer: Posts by the Center for Global Development reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. Likewise, views expressed do not necessarily reflect those of the United Nations, the United Nations Development Programme, its programmes/projects or governments. The designations employed do not imply the expression of any opinion whatsoever concerning the legal status of any country, territory or area, or its frontiers or boundaries.