Urbanization – the share of urban in total population – appears to be one of the factors that associates well with COVID-19 vaccination progress. Predominantly rural countries tend to be poorly vaccinated; conversely, predominantly urban ones tend to be better vaccinated. This positive relationship is not unexpected as a powerful common factor is at play: the level of development. But there is more to it than that and other factors such as the greater logistical challenge of reaching everyone in less urbanized settings play a role too.
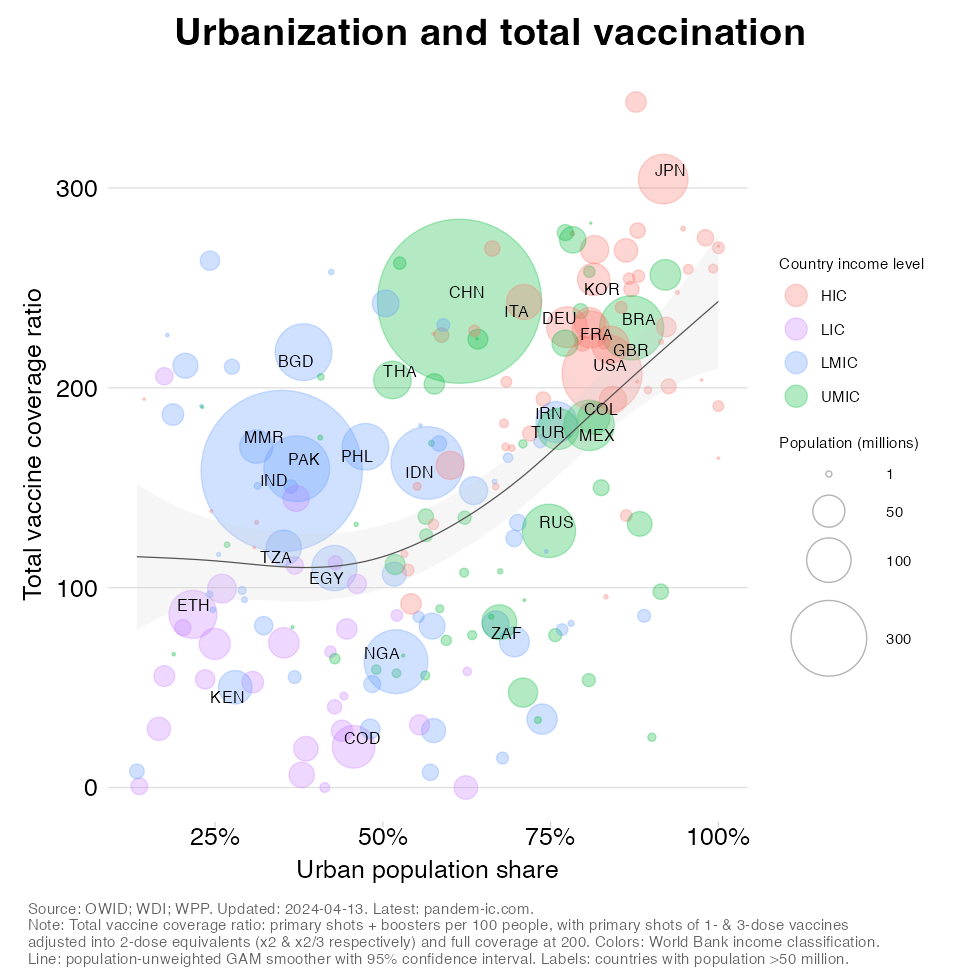
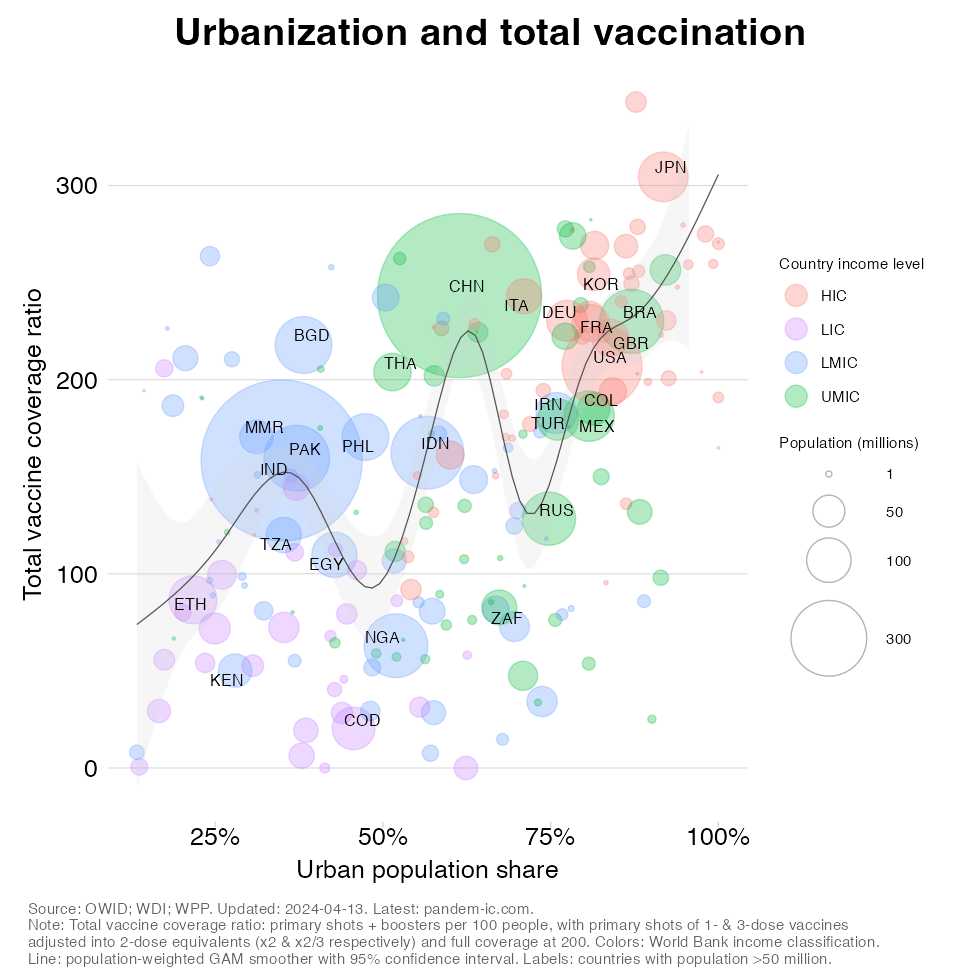
In what follows, we present the evolving relationship between urbanization and vaccination progress over time. We will let time run from the beginning of the global vaccination campaign, which we take to be December 2020, and let it pass in 2-week increments up to the present day. The regression line is weighted by population. The chart is otherwise the same as the ones presented before.
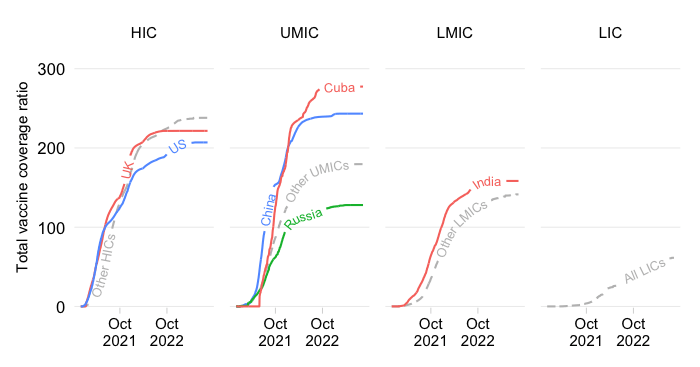
The dynamic visualization confirms the broadly positive but discontinuous relationship. It shows that, initially, when the primary series was rolled out, the low-urbanization countries made little headway, with exception of India, which dramatically pulls up the average. The progress made by China is spectacular throughout the visualization. As a result, the discontinuities discussed before carry through the entire time period. It is as if the relationship steepens somewhat initially but then gradually shifts up.
The positive association between urbanization and vaccination reflects the common influence of the level of development, which tends to raise both urbanization and vaccination. It also reflects the lesser logistical difficulties to vaccinate everyone in more urban settings. And a host of other factors may have contributed to the positive relationship, including urban-rural connectivity, rural density and perceptions of reduced vulnerability due to remoteness.
Two important outliers pull the averages up: China and India. These population giants have outperformed on vaccine coverage relative to countries at similar levels of development and similar levels of urbanization. This partly reflects their special status as vaccine manufacturers, which has been shown to benefit domestic vaccine coverage.
Disclaimer: Posts by the Center for Global Development reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. Likewise, views expressed do not necessarily reflect those of the United Nations, the United Nations Development Programme, its programmes/projects or governments. The designations employed do not imply the expression of any opinion whatsoever concerning the legal status of any country, territory or area, or its frontiers or boundaries.