Demography has had an overbearing influence over pandemic outcomes in his age-discriminating pandemic and also continues to play an overriding role in determining vaccination needs. It is important to remember this: developing countries are younger than rich countries, but they count many more elderly. That simple fact alone drives in so many ways the pandemic outcomes that we’re seeing. It also overshadows our search for solutions as we seek to vaccinate the world.
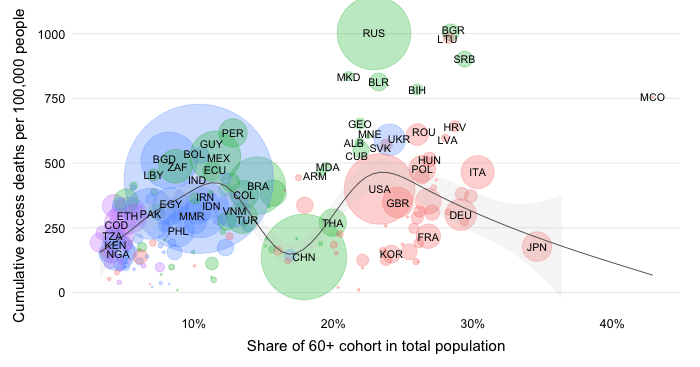
The chart below shows on the vertical axis for every country the share of the elderly cohort (seniors aged 60 and above) in the total population. Countries are grouped according to the World Bank income classification on the horizontal axes. The size of the bubbles reflects the absolute magnitude of the 60+ cohort.
We can clearly see that, on average, richer countries are a lot older in the sense that the elderly cohorts occupy a large share in total population. Development and demography are indeed closely related as this recent World Bank report develops in detail. Note however also that while there is a clear downward trend in the elderly share as one navigates from high to low income levels, there is also considerable variation within each income group.
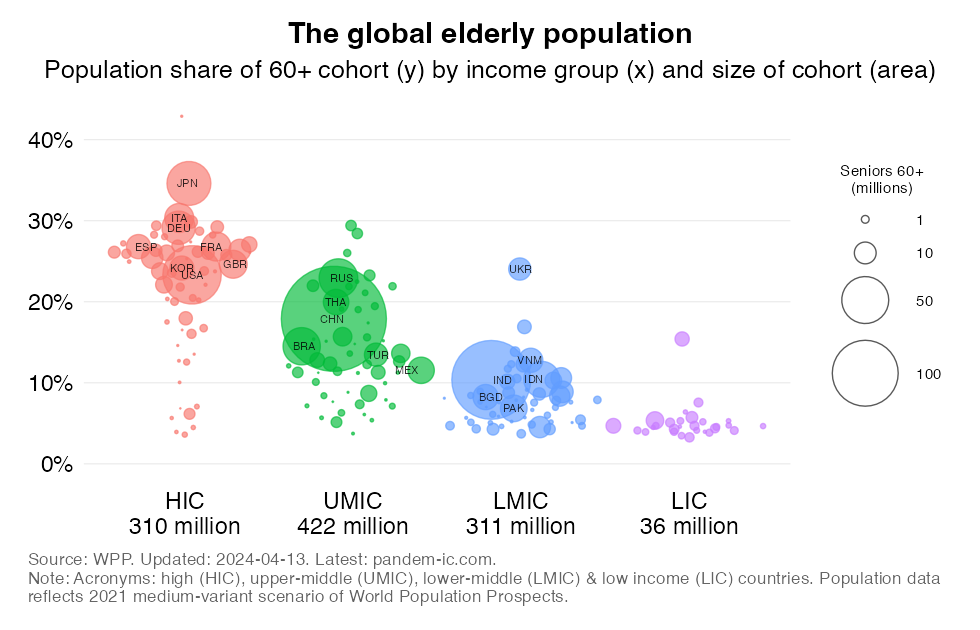
Let’s now look at the absolute picture. The byline to the X-axis legend shows the absolute size of the elderly cohort for each income group. One thing is immediately obvious. Due to their sheer population size, the developing world (UMICs, LMICs and LICs together) account for many more elderly than the rich world (HICs). HICs account for about 310 million 60+ people. UMICs and LMICs are above that. LICs, however, are considerably below that number.
The bubbles provide further granularity at the country level. Their size as mentioned represents the absolute magnitude of the elderly cohort. Here’s the top 3 countries with the largest 60+ age cohorts for each income group:
LICs: Ethiopia (6 million), DRC (4 million) and North Korea (4 million).
Interestingly, the 60+ cohort of India (144 million) is 3 times larger than that of Japan (44 million), which is the country with the second-oldest population in the world. Note that the country with the oldest population is Monaco: the 60+ population share is 43%.
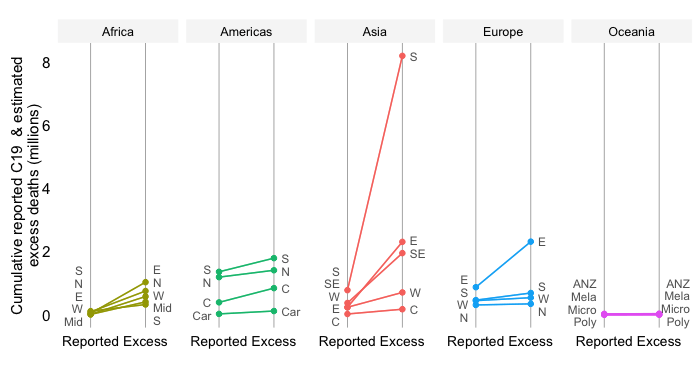
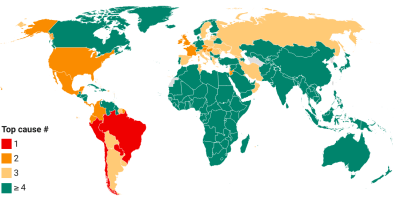
The key demographic variables that affect pandemic outcomes, including mortality, are population size and age structure.
All else equal, population size will raise the absolute mortality toll, where as age structure will affect the relative mortality roll (the mortality rate, or the absolute number of deaths per capita). The latter is the direct result of COVID-19 being an age-discriminating disease, with infection fatality rates rising sharply with age particularly beyond the 60+ category.
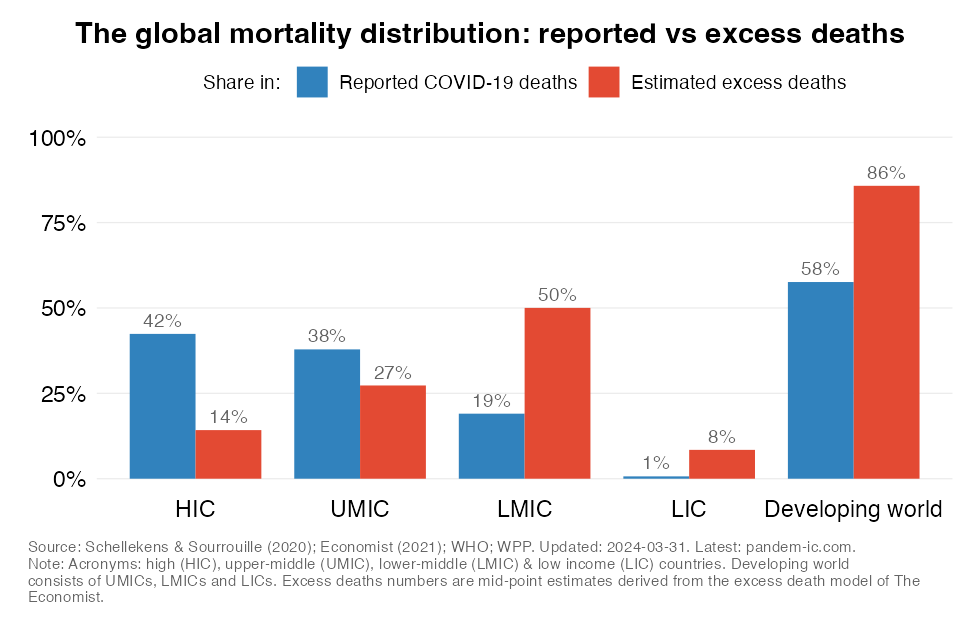
Developing countries are younger than rich countries, but their population size in the aggregate is so much larger and the absolute number of elderly people is also much larger.
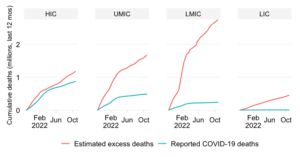
It therefore is not surprising that the developing country share in cumulative COVID-19 mortality is very elevated as the above chart shows (in blue). A similar but even more drastic picture obtains when we estimate excess deaths (in red). A detailed discussion of these results can be found in this blog.
One other reason why demography matters greatly has to do with vaccine equity as we search for solutions to the pandemic. Population size determines in this context the overall potential demand for vaccines (abstracting from issues such as vaccine hesitancy), whereas age structure determines in large part prioritization of any vaccination program (as we would ideally wish to target the elderly among the priority population).
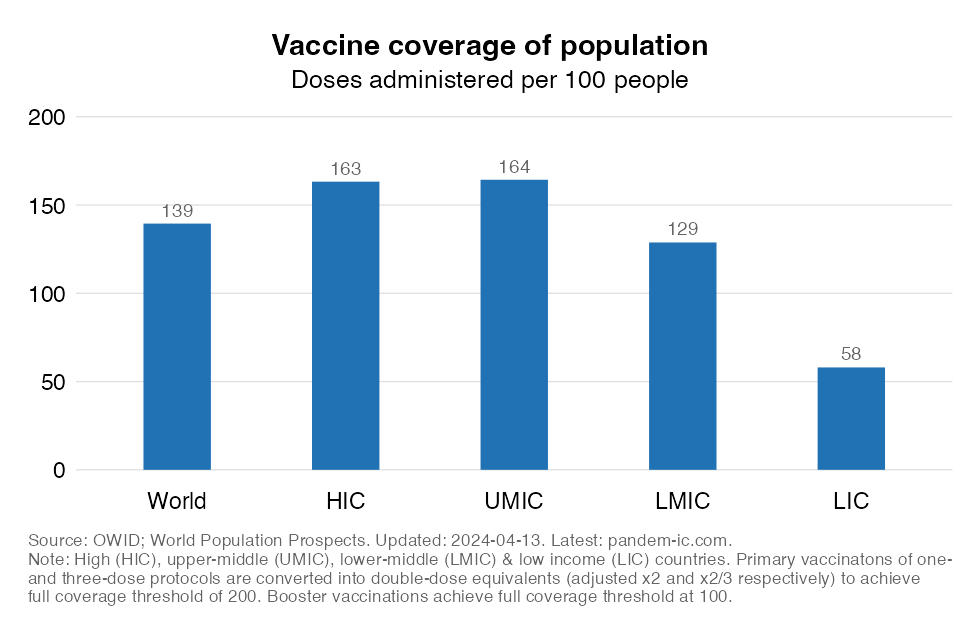
From a total population vaccine coverage perspective, the chart above is concerning. it shows that vaccination progress has not kept up with populous parts of the world. Note that the global population as per the 2021 medium-variant scenario of World Population Prospects is estimated at 7.9 billion and is distributed as follows across the World Bank income classification: 1.2 billion in HICs; 2.6 billion in UMICs; 3.4 billion in LMICs; and 0.7 billion in LICs.
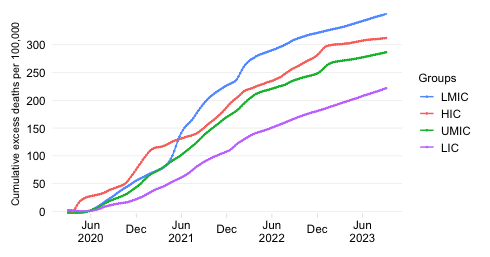
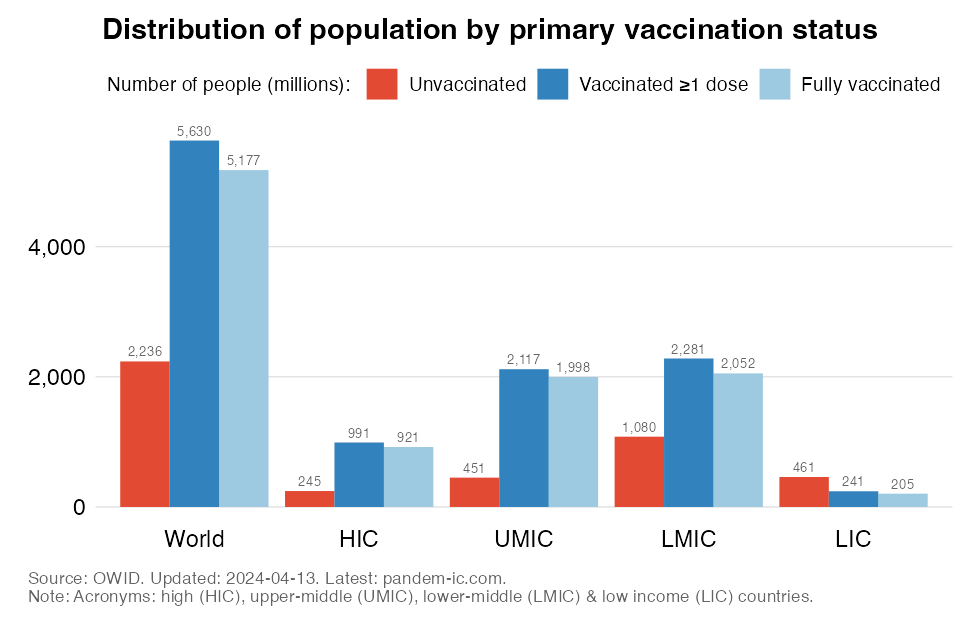
Given the low (primary and booster) vaccination rates in LMICs (which together represent 52% of the world population), many people in these countries remain unvaccinated as the chart below shows.
From an age structure perspective, there is a second concern when it comes to the global vaccination progress. The two charts below below shows the sufficiency of primary vaccines (first chart) and boosters (second chart) for the priority group, which includes here not only the 60+ cohort for each and every country but also the health workers in that country of ages 60 and below (to avoid double counting). The measure shows the extent to which the doses that have been administered to the total population are sufficient to be able to cover fully the priority group.
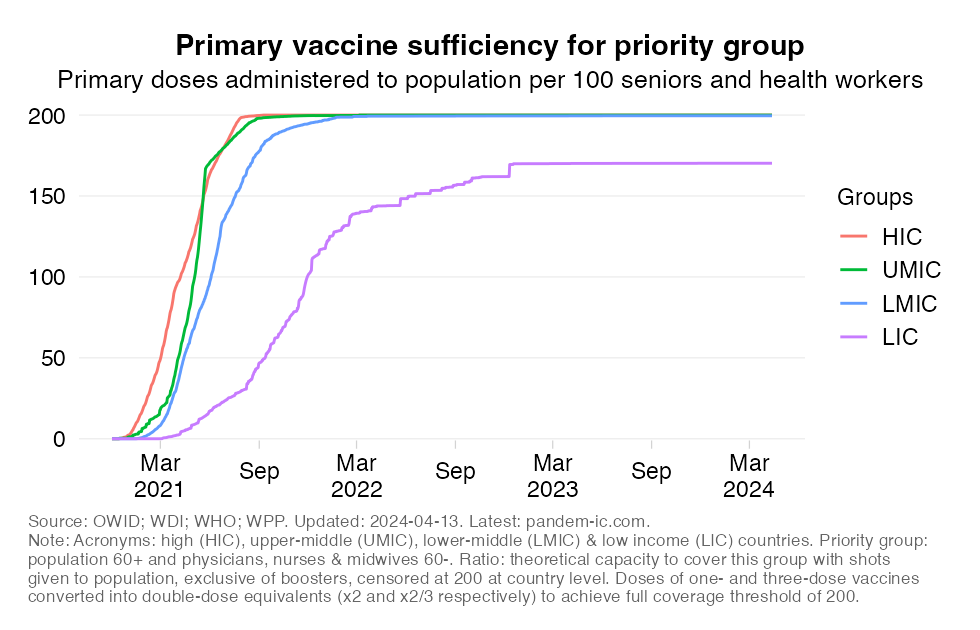
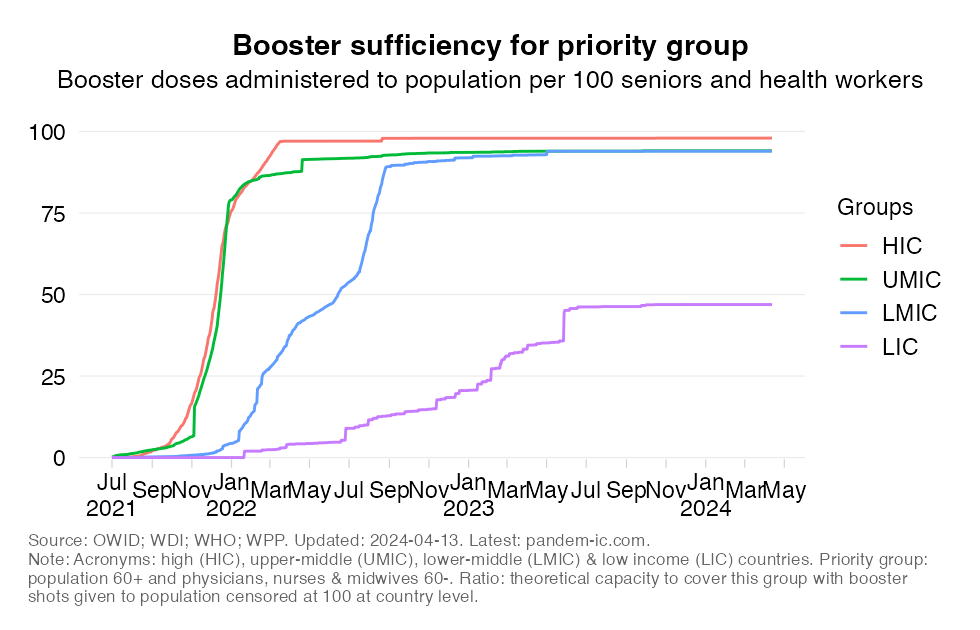
The charts show how lower-income countries have systematically lagged in their ability to cover their priority groups. They also show that even today primary doses administered are insufficient to fully cover the generally small priority group population of low-income countries. With respect to booster sufficiency, we observe still considerable shortfalls for both lower-middle-income and especially low-income countries.
Demography matters a whole lot as we try to understand the impact of the pandemic and try to implement a solution for it. Purely on the basis of demography alone (which encompasses population size and age structure) we can isolate the important role that it plays in influencing mortality outcomes. That of course is neither fate nor destiny: with good policies, countries with large elderly shares can avoid bad outcomes – and vice-versa.
Demography is also a key underpinning of the need for greater vaccine equity. Developing countries are populous and need lots of vaccines. Despite the younger age structure, there are many elderly people in the developing world, who deserve our fullest attention.
Disclaimer: Posts by the Center for Global Development reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. Likewise, views expressed do not necessarily reflect those of the United Nations, the United Nations Development Programme, its programmes/projects or governments. The designations employed do not imply the expression of any opinion whatsoever concerning the legal status of any country, territory or area, or its frontiers or boundaries.