This blog was originally published at Brookings and later at OECD and is reposted here.
“Has global health been subverted?” This question was asked exactly a year ago in The Lancet. At the time, the pandemic had already spread across the globe, but mortality remained concentrated in richer economies. Richard Cash and Vikram Patel declared that “for the first time in the post-war history of epidemics, there is a reversal of which countries are most heavily affected by a disease pandemic.”
What a difference a year makes. We know now that this is actually a developing-country pandemic—and has been that for a long time. In this blog, we review the officially published data and contrast them with brand new estimates on excess mortality (kindly provided by the folks at the Economist). We will argue that global health has not been subverted. In fact, compared to rich countries, the developing world appears to be facing very similar—if not higher—mortality rates. Its demographic advantage of a younger population may have been entirely offset by higher infection prevalence and age-specific infection fatality.
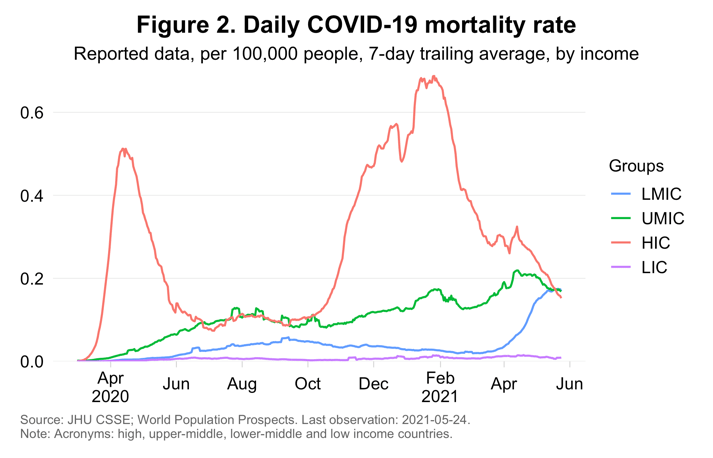
The statement that this is a developing-country pandemic is not self-evident when we look at the official statistics (Figures 1 and 2). When it comes to per capita mortality, the official data suggest that the pandemic has been most intense in high-income countries (HICs). Cumulative mortality rates and—with a few exceptions—daily mortality rates have been higher for richer countries. Most people don’t look any further and decide that HICs have suffered more.
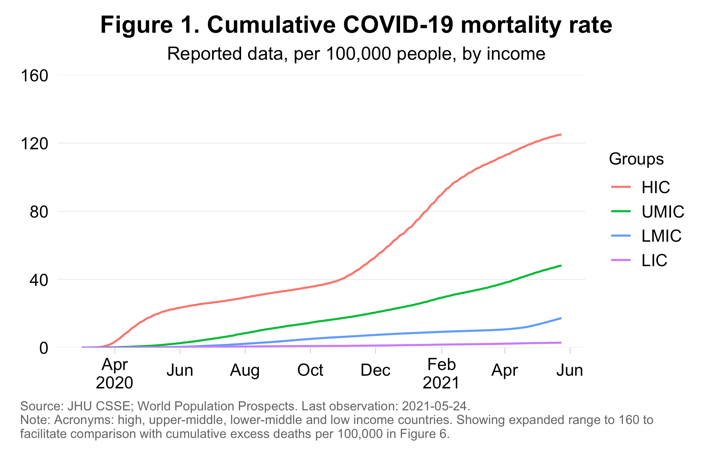
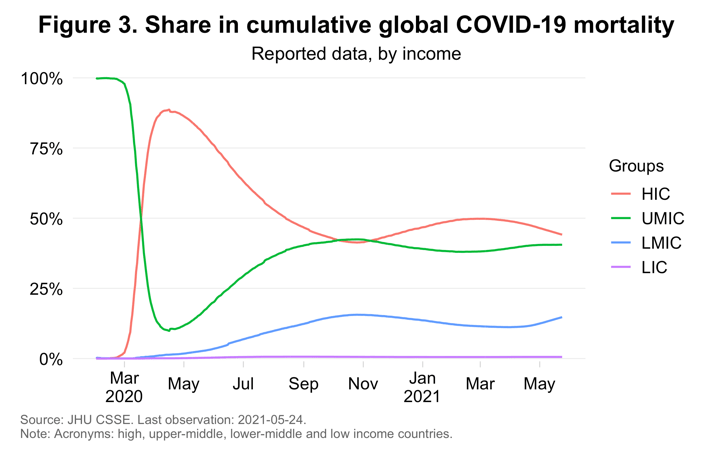
But it is necessary to also consider mortality shares. Mortality rates measure intensity, which highlights country performance, but they do a poor job in reflecting the contribution to global mortality. Given that the developing world is both younger and more populous than the HICs, we would expect its mortality rates to be lower and its mortality shares to be higher. Official data indeed show that the developing-country share in cumulative mortality is high: slightly above 50 percent (Figure 3).
This wasn’t always the case: The global mortality distribution has seen big swings since the onset of the pandemic. One upper-middle-income country (UMIC) dominated the global death toll initially: China. Soon after, outbreaks in HICs lifted their share in global mortality to almost 90 percent. A shift to UMICs followed, then quickly to lower-middle-income countries (LMICs). When winter came to the northern hemisphere, a new wave drove up the HIC share. More recently it has again started to recede. Throughout the period, the reported share of low-income countries (LICs) remained negligible.
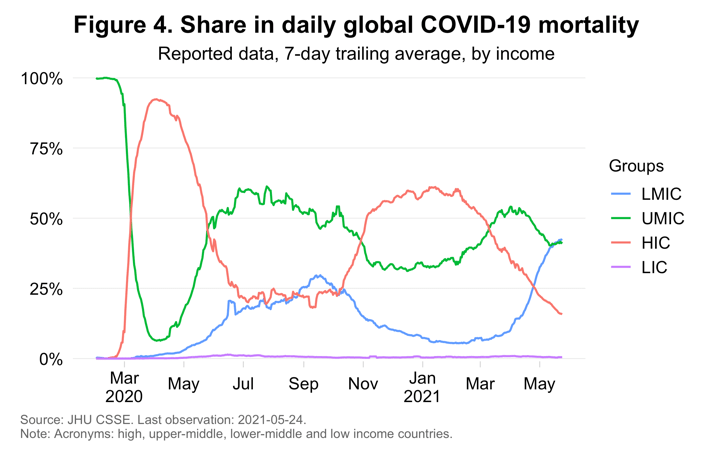
The daily mortality distribution puts into sharper focus the most recent trends (Figure 4). The good news is that, in part thanks to vaccines, HIC mortality rates have plummeted. The bad news is that rates have spiked in LMICs and remain at high levels in UMICs. As a result, 2021 saw a complete shift in the daily mortality distribution: The LMIC share rose from 7 to 42 percent; the UMIC share from 33 to 42 percent; and the HIC share dropped from 59 percent to 15 percent—a trend that may become more pronounced in coming months.
The Economist has just published new estimates of excess deaths. Excess deaths measure the difference between observed and expected deaths throughout of the pandemic. Previously confined to mainly the richer countries, excess deaths are thanks to the new estimates available for the entire world. A gradient-boosting machine-learning algorithm helped fill the data gaps on the basis of 121 predictive indicators that are comprehensively available. With this method, global excess deaths are estimated at 7 million to 13 million, with 10 million as the midpoint.
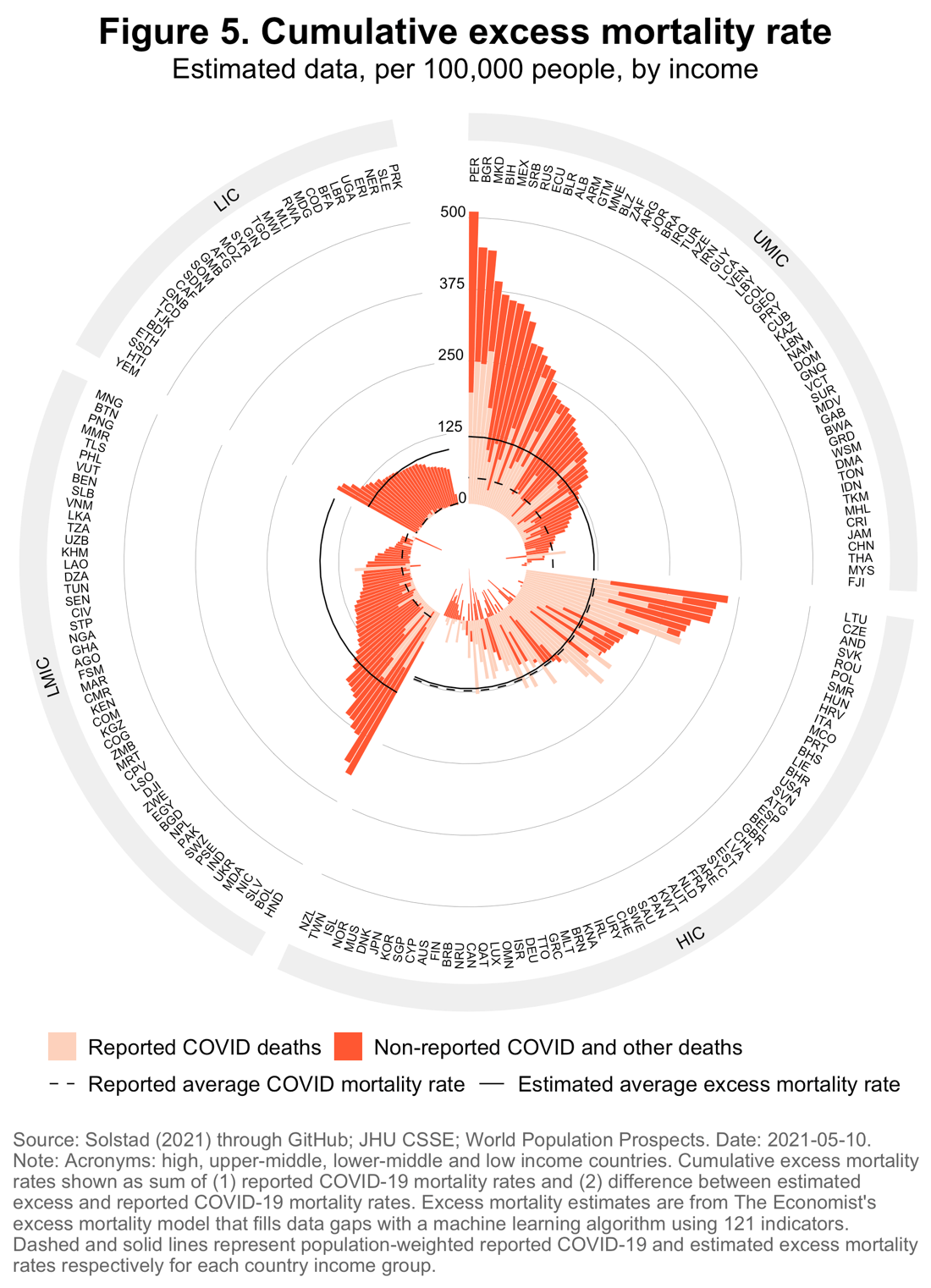
Figure 5 shows the detailed results by World Bank income classification. Two patterns are striking.
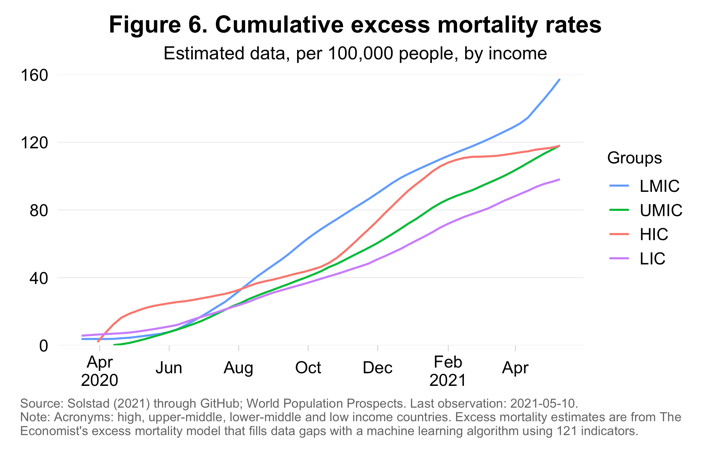
First, excess mortality rates for the developing world are much higher than what reported COVID-19 mortality data suggest: 2.5 times higher for UMICs, 12 times more for LMICs, and 35 times greater for LICs. For HICs they are practically the same—actually about 3 percent lower. To see this, compare the dashed and solid lines, which represent the population-weighted averages for each income group (see also Figure 6 for the time series).
Second, non-reported COVID-19 deaths and other excess deaths are much larger than reported COVID-19 deaths especially in poorer countries (compare the darker and lighter shades of each bar). The small gap for HICs may reflect the opposite effects of inadequate testing and “general equilibrium” impacts of the pandemic (such as the vanished flu season).
Perhaps the most striking result is the compression of mortality rates across income groups (Figure 6). Mortality rates in LMICs are the highest (157), then UMICs and HICs (both 118) and then LICs (98). But relative to the dispersion seen in the reported COVID-19 mortality rates (Figure 1), one could say they’re “about the same.” These estimates are subject to uncertainty, but the 95% confidence intervals are considerably above the reported COVID-19 mortality rates, particularly among UMICs and LMICs (which together represent 75 percent of the world’s population).
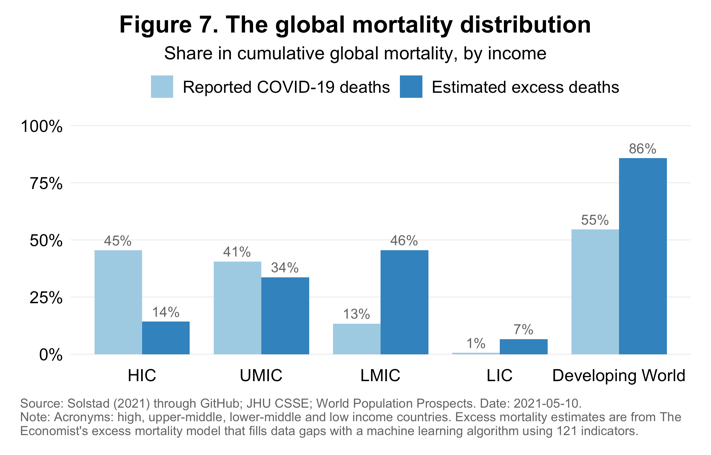
The midpoint estimates entail a completely different mortality distribution (Figure 7). If the midpoints hold true, the developing world may account for 86 percent of global mortality (as of May 10). This compares to a share of 55 percent using officially reported data. The biggest increases are in the share of LMICs and LICs.
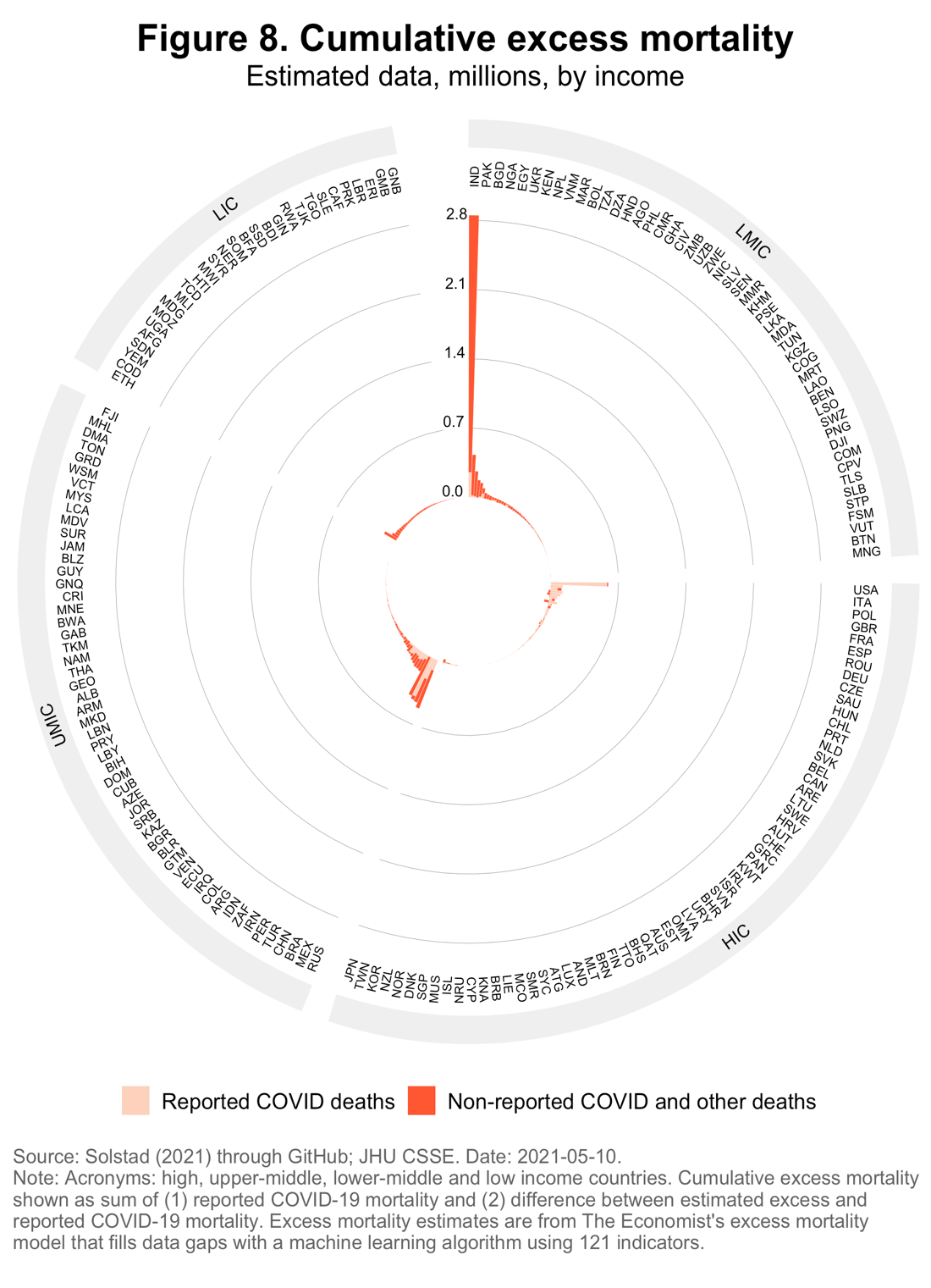
While virtually all developing countries are contributing to the rise (see Figure 5), rising mortality rates in the developing world’s most populous countries will produce the largest absolute impact on global mortality. We can see this very vividly in Figure 8, which shows the cumulative death toll in millions of souls. The tragedy that continues to unfold in India has claimed a very large death toll of close to 3 million. While considerable uncertainty surrounds these estimates, alternative methods suggest they are in the ballpark.
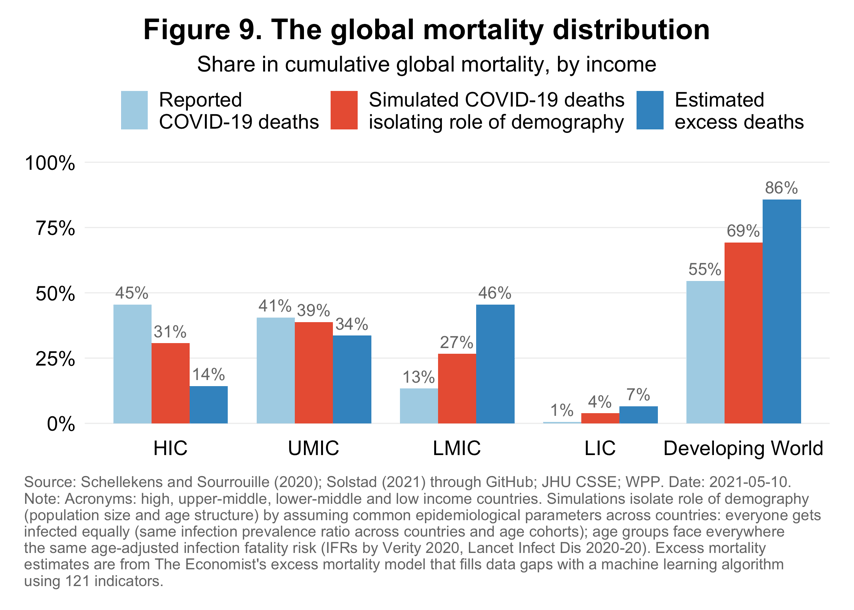
It is useful to do a thought experiment (Figure 9). Imagine all countries—rich and poor—faced the same epidemiological odds; that is, suppose that everyone has the same chance of getting infected and everyone faces the same age-specific fatality rates. Under these conditions, we would capture the pure effect of demography on the mortality distribution and obtain an estimate of the demographic advantage of the developing world.
In such a scenario, we expect the developing-world share in global mortality to be around 69 percent (Figure 9, middle bar in red). Applying common epidemiological parameters to the developing world boosts their share in global mortality because of the large absolute numbers of elderly. Though developing countries are younger, they are much more populous. As a result, the 60+ population of the developing world is 2.4 times larger than its counterpart in HICs. India alone, for example, counts 140 million people over 60; this is three times the number in Japan, which has the world’s oldest population after Monaco.
The generally younger age distributions of the developing world were believed to protect against a pandemic that discriminated against older people. The fact that the excess mortality shares (Figure 9, dark blue bar on the right) are significantly higher suggests that developing countries have likely squandered their demographic advantage as mortality is higher than demography alone would indicate. In other words, developing countries likely face worse epidemiological odds in the form of higher infection prevalence and/or more elevated age-specific infection fatality risk.
We can think of many structural reasons why that would be the case. Infection prevalence has likely been fueled by environmental factors such as urban density as well as poverty and informality, which complicate physical distancing. Over 1 billion people, mostly in developing countries, live in slums. Flattening the curve will therefore be more difficult in many developing countries, meaning that preexisting health capacity constraints will become binding more quickly.
Age-specific infection fatality rates are also likely more elevated than in HICs. Comorbidities are highly prevalent in the developing world. Of the 1.1 billion people with hypertension, two-thirds live in developing countries. Over the last decade, the number of cases and prevalence of diabetes has risen most quickly in the developing world. Moreover, limited access to quality health care in developing countries would mean that many ailments would be left untreated or undertreated, heightening vulnerability.
Official data point to a big shift in the mortality distribution to the developing world in recent months. Excess death estimates suggest that developing-country shares have been much higher than previously thought. Regardless of what the precise channels have been, one conclusion is clear: This is now—and has for a long time been—a developing-country pandemic.
Note: Indermit Gill is Chief Economist of the World Bank Group and Nonresident Senior Fellow at Brookings. Philip Schellekens is Senior Economic Advisor at IFC – World Bank Group. The authors are grateful to Sondre Solstad, who produced the excess death estimates at The Economist, for making additional results by World Bank income groups available to us.
Disclaimer: Posts by the Center for Global Development reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. Likewise, views expressed do not necessarily reflect those of the United Nations, the United Nations Development Programme, its programmes/projects or governments. The designations employed do not imply the expression of any opinion whatsoever concerning the legal status of any country, territory or area, or its frontiers or boundaries.





